Intracytoplasmic Sperm Injection (ICSI)
What is intracytoplasmic sperm injection?
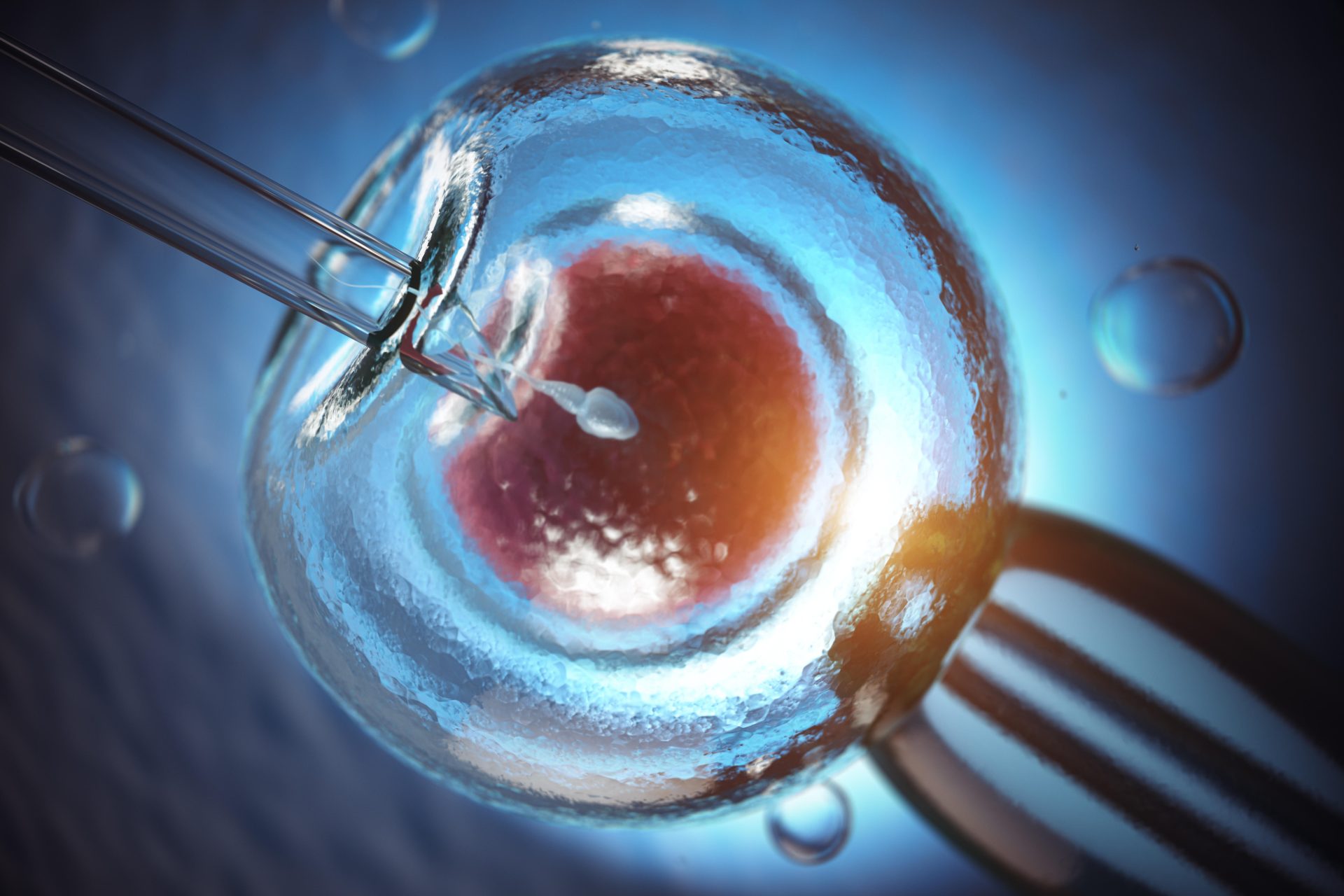
Intracytoplasmic sperm injection (ICSI) is a laboratory method of fertilizing eggs with sperm, where the embryologist selects under a high-resolution microscope a sperm with normal morphology and vigorous progressive motility, aspirates it into a special syringe, and then injects it into an egg.

Who needs to undergo ICSI?
ICSI is primarily directed at couples where sperm quality is not good enough for classical IVF to be performed. Examples of such cases include:
- Patients with low sperm count, low motility, or low number of morphologically normal sperm, or a combination of the above
- Patients whose sperm lack an acrosome (which is necessary for natural penetration of sperm into the egg)
- Patients who cannot ejaculate or exhibit retrograde ejaculation
- Patients where sperm collection is performed directly from the testes or epididymis by aspiration or biopsy (e.g., in azoospermia due to obstruction or not)
- Patients undergoing IVF after egg cryopreservation
- Patients undergoing preimplantation genetic testing
Also, ICSI may be indicated in:
- Patients in whom the use of classical IVF resulted in low fertilization rates
- In cases of using donor sperm (either due to sperm quality or to reduce the quantity of sperm to be thawed and used)
What procedure is required for ICSI?
As with classical IVF, before ICSI the following stages are required:
1) Ovarian stimulation with medications to develop and collect more than one egg. Collection of multiple eggs (when feasible) ensures maximum IVF effectiveness, and modern stimulation strategy involves attempting to collect as many eggs as possible using patient-friendly stimulation protocols. Typical ovarian stimulation usually lasts 10-12 days (8-14 days).
2) Monitoring: During stimulation, typically 2-3 visits to the Fertility/Reproductive Medicine specialist will be required for hormonal (blood draw) and ultrasound examination (transvaginal ultrasound). These tests allow the physician to monitor the smooth progress of ovarian stimulation and estimate the number of eggs to be retrieved.
3) Completion of stimulation and egg retrieval: When the physician observes on ultrasound a group (usually >2) of follicles of adequate size (usually ≥17mm in mean diameter), final oocyte maturation proceeds with administration of a final injection. Egg retrieval is usually performed 36 hours (34-38 hours) after this injection. Egg retrieval is performed under sedation (a form of general anesthesia), without pain, and usually lasts 20-40 minutes. It involves retrieving eggs under ultrasound guidance through a relatively thin needle that passes through the thin vaginal wall and aspirates fluid from each follicle. After egg retrieval, patients may feel some discomfort similar to menstrual cramps and may have a small amount of vaginal bleeding. These symptoms usually resolve completely within 24-48 hours.
After egg retrieval, it is necessary to perform egg cleaning from cell layers (cumulus cells) that surround them and make ICSI difficult. Removal of cumulus cells (denudation) is performed in the laboratory either chemically or mechanically.
The next step is to check the maturity of the eggs, which is done 1-4 hours after egg retrieval. Mature eggs are those that have already expelled the first polar body and are at the Metaphase II stage. These eggs are ready to be fertilized by sperm. Eggs that are not mature cannot be used for ICSI.
At the same time, sperm processing is performed to find morphologically normal and motile sperm. This process can be particularly time-consuming, especially if the number of such sperm in the semen is very small. Once the appropriate sperm is found, it is immobilized and aspirated using a microscopic syringe (pipette) and then carefully injected into the mature egg. The process of injecting the sperm into the egg usually takes 1-2 minutes per egg.
What are the ICSI success rates?
The success of ICSI is initially assessed by evaluating the number of eggs showing signs of successful fertilization 16-18 hours after ICSI. Generally, we expect approximately 65% of eggs to have been successfully fertilized, although these rates may differ depending on sperm quality, egg quality, and the technical skill/experience of the embryologist who performed the ICSI.
Is ICSI safe?
ICSI is an additional, highly technical step in the IVF procedure (a form of microsurgical intervention on the egg), and therefore there is a theoretical risk of egg damage from manipulations during intracytoplasmic sperm injection. Most studies conducted, however, show that in the hands of properly trained embryologists, the method is safe for the egg.
Also, large epidemiological studies support that children born after ICSI have a slightly increased risk of congenital anomalies. This increase is particularly observed in boys and concerns congenital anomalies of the urogenital system. The current scientific view is that this increase is mainly due to genetic errors in the child’s father, which also constitute the cause of male infertility requiring ICSI use. These genetic errors will subsequently affect, in a small percentage, the way the urogenital system of the male embryo will form and will lead to the appearance of such congenital anomalies.
Recently, however, new scientific evidence suggests that the ICSI procedure itself may also be partially responsible for a small increase in the risk of congenital anomalies. For this reason, ICSI use should only be performed when there are clear medical indications and the benefits outweigh the small theoretical risks.
In conclusion, the ICSI procedure has been used for more than 30 years and has helped millions of couples achieve their own biological child. It is a highly valuable and safe method when used for appropriate medical reasons by experienced personnel.